For healthcare providers and family caregivers, “managing” symptoms and behaviors that arise in a person living with dementia requires patience and compassion, and sometimes, the skill of a detective. To successfully manage a challenging behavior, caregivers must try to understand what is causing the behavior. Very often, it is due to some sort of unmet need.
2.1 Symptoms and Behaviors Associated with Each Stage of Dementia
A symptom is a change in the body or the mind. Symptoms change as a person’s dementia progresses, often leading to changes in a person’s behavior. For some people symptoms associated with dementia worsen quickly while for others, symptoms progress more slowly.
We associate certain symptoms and behaviors with stages. But keep in mind that the type of dementia, along with a person’s general physical and psychological health can affect symptoms and behaviors as much as the stage of a person’s dementia.
2.1.1 Mild Dementia
In early, mild Alzheimer’s disease, plaques and tangles appear in the part of the brain responsible for memory and learning. This part of the brain is called the hippocampus. It converts recent, short-term memories into long term memories by storing, organizing, and retrieving memories.

Location of the hippocampus. Source: Image courtesy of the National Institute on Aging/National Institutes of Health. Public domain.
The inability to recall something that just happened (short-term memory) is a common symptom in the early stage of Alzheimer’s disease and other types of dementia. A person can also have difficulty understanding where they are in relation to nearby objects (visual-spatial memory), have trouble finding words (verbal memory), and may not remember certain facts or experiences.
In the early stage, logical thinking, language, and judgment are often mildly affected. For example, a person may forget things more often than they did in the past or have trouble following a complex conversation.
Brain Changes in Mild Dementia
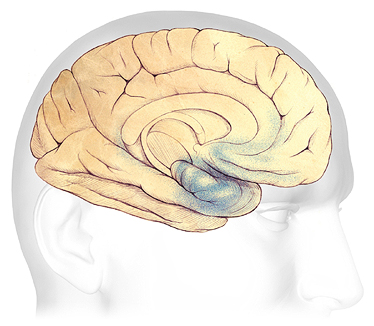
In early AD, sometimes before symptoms can be detected, plaques and tangles begin to form in and around the hippocampus (shaded in blue). Source: The Alzheimer’s Association. Used with permission.
Even when symptoms are mild, a person’s behavior can begin to change, especially in Alzheimer’s disease and some other types of dementia. People often know something is wrong and may try to hide their mild confusion from friends, coworkers, and family. This can lead to depression, stress, mood changes, and anxiety.
2.1.2 Moderate Dementia
As symptoms associated with dementia progress to the moderate stage, plaques and tangles spread forward to the areas of the brain involved with language, judgment, and learning. Many people are first diagnosed with Alzheimer’s or another type of dementia at this time.
During this stage, work and social life become more difficult. A person’s judgement and logical thinking may be affected. Damage affects the areas of the brain involved with:
- speaking and understanding speech
- safety awareness
- planning and sequencing tasks
- ethical thinking
Brain Changes in Moderate Dementia
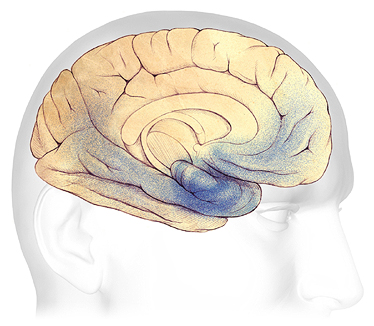
As symptoms progress from mild to moderate, plaques and tangles spread from the area of the hippocampus (dark blue) forward to the frontal lobes (shaded in light blue). Source: The Alzheimer’s Association. Used with permission.
Because of memory problems and confusion, a person living with moderate dementia may find daily tasks more difficult and will very likely need help with personal finances, medications, and medical management.
In the moderate stage, behavioral changes become more obvious to caregivers. Some people may begin to repeat questions, call out, or repeatedly demand your attention. Sleep problems, anxiety, and agitation can develop.
A person living with moderate dementia is usually still able to walk. This is because the part of the brain that controls movement is not affected. A caregiver may need to provide more direct monitoring of daily activities and the person living with dementia may no longer be safe on their own.
2.1.3 Severe Dementia
Behaviors that emerged in the middle stage, when executive functioning and communication abilities typically decline, continue in the severe stage. In the severe stage, an individual living with dementia may become increasingly nonverbal, and mobility challenges can become more pronounced.
In severe Alzheimer’s disease, because so many areas of the brain are affected, the ability to care for oneself is severely affected. Confusion, indecisiveness, sleep disturbances, and emotional outbursts are very common.
Brain Changes in Severe Dementia
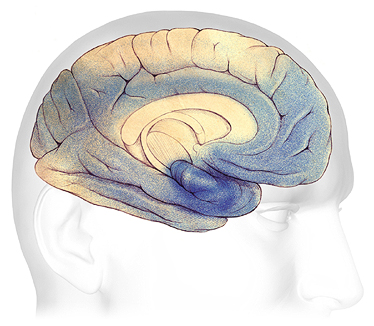
In advanced Alzheimer’s, plaques and tangles have spread throughout the brain (shaded in blue). Source: The Alzheimer’s Association. Used with permission
All sorts of challenging behaviors can occur at this stage, especially if caregivers (including professional caregivers) are poorly trained, easily frustrated, or highly stressed. A person living with severe dementia may wander, rummage, or hoard. Screaming, swearing, crying, shouting, loud demands for attention, negative remarks to others, and self-talk are common. These outbursts are often triggered by unmet needs such as frustration, boredom, loneliness, depression, cold, heat, loud noises, or pain.
A person experiencing severe dementia loses a great deal of independence, and around-the-clock care may eventually be needed. Caregivers will likely need to oversee and directly assist with eating, bathing, walking, dressing, and other daily living activities.
2.1.4 Symptoms and Behaviors at the End of Life
As someone nears the end of their life, they may be completely dependent on caregivers. If they are unable to communicate their needs and desires using speech, caregivers must learn to recognize non-verbal cues. A person at this stage may be bedridden or nearly bedridden.
Immobility, swallowing disorders, and malnutrition can occur. Because people at this stage are much less active than in earlier stages of dementia there is an increased risk of developing acute conditions that can lead to illness or death. Pneumonia, the most common cause of death among older adults who have Alzheimer’s or another type of dementia, is a particular concern.
At the end of life, it is likely that both short- and long-term memory are affected. Sensory changes such as loss of vision and hearing mean a person can be startled by loud noises and quick movements. Depending on the type of dementia, a person may experience agitation, psychosis,* delirium,** restlessness, and depression.
*Psychosis: loss of contact with reality.
**Delirium: a sudden, severe confusion that can be caused by infections, a reaction to medications, surgery, or illness.
2.2 General Problem-Solving Approach to Challenging Behaviors
Problem solving is an important skill for caregivers and healthcare providers to develop when working with a person living with dementia. Compassion, reassurance, and active listening can reduce or even prevent many challenging behaviors. These practices can also reduce the use of antipsychotics and other medications often used to manage challenging behaviors.
The “ABC” model emphasizes data gathering and problem-solving. This approach helps providers and caregivers understand when and how often a particular behavior occurs. It is particularly effective when successful strategies are shared by staff, caregivers, and family members.
The ABC Approach considers:
- A (Antecedent) What caused the behavior?
- B (Behavior): What is the behavior?
- C (Consequence): What are the consequences of a behavior?
The ABC approach also encourages caregivers and healthcare providers to examine their own behaviors and responses. Understanding your own biases, frustrations, and triggers helps you approach a person struggling with dementia with patience and compassion.
2.3 Strategies for Addressing Common Challenging Behaviors
Addressing common challenging behaviors in a person living with dementia requires training, strategies, and techniques that change as a person’s symptoms and behaviors change. Because dementia is progressive, strategies that work with mild dementia may not work in the later stages of dementia.
Good management means creating a safe and comfortable physical environment, learning how to divert the person’s focus to a meaningful activity, and encouraging regular physical activity and social engagement. For a person living with dementia, negative environmental influences, frustration, boredom, pain, or untreated medical or medication issues create can lead directly to challenging behaviors.
Although not a comprehensive list, certain behaviors are common in people living with dementia. This includes agitation, aggression, psychosis, wandering, rummaging, hoarding, and sleep disturbances.
2.3.1 Agitation and Aggression
Agitation, aggression, and psychosis are labels on behaviors that are often caused by environmental or personnel approaches rather than being due entirely to the person’s brain changes. These reactions should be viewed as an expressive communication of a possible unmet need.
Teepa Snow, STOP Treating Behaviors with Restraining Medications
Agitation and aggression are among the most common and challenging symptoms in older adults living with dementia. These behaviors worsen a client’s daily functioning, increase the risk of injury, and increase the likelihood of hospitalization and long-term care placement. They also impose a significant burden on caregivers and healthcare providers (Lichwala et al., 2026).
Agitated behaviors can include:
- Irritability and worry
- Restlessness, unable to settle down
- Pacing
- Repetitive behaviors
- Confusion
- Loud demands
- Obscene language
Aggressive involves physically or verbally threatening behaviors. This can include:
- Hitting, punching, kicking, pushing.
- Throwing objects or using objects to hit or lash out.
- Engaging in inappropriate sexual advances or touching.
- Client-to-client aggression, verbal aggression.


Left: An older woman living with dementia expresses her frustration and anger. Right: An older man living with dementia lashes out at his caregiver. Source: created by author using Midjourney AI.
In assisted living facilities, resident to resident aggression is not uncommon with verbal aggression being the most common type of aggressive behavior. A study of several assisted living facilities in New York found that aggressive behaviors were more common among residents of memory care units (Pillemer et al., 2024).
Agitated and aggressive behaviors often occur during personal care tasks involving close contact. A person may feel threatened or feel their personal space is being violated. Depending on the type and severity of a person’s cognitive changes, agitated and aggressive behaviors can become more pronounced as a dementia progresses.
To manage aggressive behaviors, staff and caregiver training are essential. Psychosocial and environmental interventions, and recognition of personal habits and patterns can reduce or even eliminate agitated or aggressive behaviors.
When you encounter agitated and aggressive behaviors, take a deep breath, slow your movements, and be respectful of personal space. Always introduce yourself before entering a person’s room. When you approach a person who is agitated:
- Speak calmly and actively listen to their complaints or frustrations.
- Reassure the person that they are safe.
- Try to distract the person by offering an activity or chore.
- Try to reduce noise and clutter.
- Consider physical and medical causes of a person’s agitation.
Antipsychotics are often used to treat agitated and aggressive behaviors in people living with dementia. They should be used for the shortest possible time and only as a last resort.
Charles Lashes Out at Frances
Background: Frances, a physical therapist working in an assisted living facility, was helping Charles go from his room to the activities room. Charles, seated in his wheelchair, was quiet and relaxed as they moved down the hall.
Antecedent: In the hallway outside the activities room, Frances was stopped by two co-workers who engaged her in a conversation about another resident. All three were standing behind Charles, talking animatedly.
Behavior: Frances placed her hand on Charles’s shoulder to try to include him in the conversation and he angrily pushed it away, yelling in a loud voice “Stop that!” When one of Frances’s co-workers tried to calm him down, Charles yelled again and struck out at the co-worker.
Consequence: Instead of ignoring Charles and talking over him, the physical therapist should have stopped, kneeled down beside Charles, offered her upturned hand, and introduced her colleagues. She should have asked Charles if she could talk for a moment with her co-workers and included him in the conversation. Better yet, she could have asked her colleagues to wait until she and Charles finished what they were doing and continued the conversation after Charles was seated at the activities table.
Discussion: Frances and her co-workers could have avoided this incident entirely. This is a situation that didn’t need to agitate Charles. If Frances and her co-workers had been respectful of Charles and validated his needs and preferences, they could have avoided upsetting him and modeled good practice for their co-workers.
2.3.2 Dementia-Related Psychosis
Dementia-related psychosis occurs when a person experiences symptoms such as delusions, paranoia, or hallucinations. A delusion is a false belief or a misinterpretation of a situation. For example, a person living with dementia might confuse her daughter with her mother or she might accuse someone of stealing an item has simply been misplaced.
Paranoia is a type of delusion in which a person may believe—without a good reason—that someone is lying to them, being unfair, or are “out to get me.” This can cause a person to become suspicious, fearful, or jealous of other people. Paranoia often includes people close to the person living with dementia (caregivers, family members, or friends).
Hallucinations occur when a person hears, tastes, smells, sees, touches, or feels something that is distorted or not there. For example, a person may see shadows, cats running through the room, or images of threatening people or things (Fischer, 2022).
Visual hallucinations can occur in the moderate to severe stage of dementia and are particularly common in people with Lewy body dementia*. For a person living with Lewy body dementia, antipsychotic medications can make hallucinations worse.
*Lewy body dementia: a type of dementia with cognitive decline, “fluctuations” in alertness and attention, visual hallucinations, and slowness of movement, difficulty walking, or rigidity (stiffness).
The first step in the management of delusions and hallucinations is to rule out delirium or another acute medical cause. Observing a person’s behavior and listening to what they have to say often helps caregivers uncover the root cause of the delusion or hallucination.
For a person with new onset of visual hallucinations, the number one cause is medication side effects. For this reason, all medications the person is receiving should be regularly and carefully reviewed.
Acute health issues such as urinary tract infections or environmental factors such as poor lighting or sensory overload can contribute to delusions and hallucinations. Brain changes can also contribute to hallucinations, especially changes related to sensory awareness.
When communicating with someone who is experiencing paranoia or delusions, remember that the delusion is very real for that person. Do not argue or try to correct the person. Explaining the truth of the situation does not work. Do not agree or validate the paranoia or delusion—try to respond to the person’s emotion. For hallucinations, it is often helpful to decrease auditory and visual stimuli. It is also important to evaluate the person for a visual or hearing impairment.
What Do You Think?
Consider that the claims by the person with dementia may be real. Complaints of strangers entering several resident rooms and stealing items at a Florida assisted living facility were attributed to dementia, hallucinations, and paranoia by healthcare providers (including nurses and physicians). As the complaints mounted, managers decided to install cameras in the alley next to the facility. It turned out that several of the sliding glass doors facing the alley had broken locks. The cameras showed that people were indeed entering rooms at night and rummaging through residents’ drawers and closets. There truly were people entering resident rooms and stealing items!
2.3.3 Wandering
Wandering and exploring are activities we all enjoy. It can occur at any stage of a person’s dementia. But, because a person living with dementia might be at risk for falls or injury, providers and caregivers often see wandering as a problem and try to control or prevent this behavior. However, preventing a person from safely wandering creates other problems, such as boredom, loss of social interaction, stigma, loss of conditioning, pain and discomfort, and even skin breakdown.
Wandering is a common in people living with almost all types of dementia. Nearly 60% of people living with dementia will wander during the course of their disease. Wandering can happen at home or in the community. In institutional settings, wandering occurs in about 40% of clients (Anu et al., 2024).
Wandering can involve moving to a specific location, lapping, or circling along a path, or pacing back and forth. People may wander out of habit or because they are convinced something needs to be done. They may think they need to return home after work, cook dinner, walk the dog, exercise, or search for something they think they have misplaced. The most important goal is to prevent a person from wandering into unsafe areas, other residents’ rooms, or eloping* from a facility.
*Eloping: When a person wanders away or leaves a facility or home unsupervised or unnoticed.
A person who was socially and physically active throughout their life, who enjoys music, or who deals with stress by engaging in physical activities is more likely to wander than others. The habits of a lifetime and the desire to be socially active remain intact. Additionally, someone who experienced stressful events throughout their life or a person who responds to stress by engaging in physical activities is more likely to wander.
Managing wandering behaviors in a person living with dementia requires a thoughtful and creative approach. Understanding the reasons for wandering should include regular review of medications to make sure wandering is not the result of medication side effects, overmedicating, or drug interactions.
Address wandering by:
- Redirecting a person to a purposeful activity.
- Offering safe, looping wandering paths with interesting rest areas.
- Installing rails and grab bars.
- Providing regular exercise.
- Offering to wander with the person.
Engaging a person in simple chores such as folding laundry or assisting with dinner can give them a sense of purpose and fulfillment. Electronic devices attached to the person’s ankle or wrist alert staff or family members when someone has wandered out of a designated area. Subjective barriers such as grid patterns on the floor in front of exit doors, camouflage, and concealment of doors and doorknobs have been shown to discourage a wanderer from exiting a building.
For a person in the later stage of dementia, especially someone who is unable to walk safely, lowering the seat on the wheelchair allows a person to wander safely by propelling the wheelchair with their feet. If the chair cannot be lowered, a “drop seat” can be installed, which has the added benefit of allowing the addition of a good-quality pressure-relief cushion. The wheelchair should be adjusted to equalize pressure wherever a person’s body meets the seat, back, sides, or cushion. Daily skin monitoring is essential.
Did you Know. . .
For people who wander away from their home or care facility, the immediate action is to call 911. Florida maintains a Silver Alert program for cognitively impaired older adults who become lost while driving or walking. The Silver Alert program is activated by law enforcement and broadcasts information to the public so they can assist in the rescue of the endangered person and notify law enforcement with helpful information. For more information, contact the Silver Alert information line, local law enforcement, or the Florida Department of Law Enforcement either online or by phone at 888 356 4774.
The Wanderer
Mrs. Winkler lives in an assisted living facility in Miami. She is also living with moderate dementia and uses a wheelchair to get around. This morning, a caregiver asks if she would like to go to the activities room. Mrs. Winkler agrees, and the care assistant wheels her to the activities room and leaves her there. After about 20 minutes, Mrs. Winkler decides to leave the activities room. She heads down the hall and is stopped several times by staff, all of whom turn her back toward the activities room—usually with a reprimand.
As soon as the staff member is gone, Mrs. Winkler turns around and continues on her way. She stops near the elevator, where she sits for about 10 minutes watching people come and go. Several staff members pass her and sternly tell her not to get on the elevator. Each staff member leaves her in exactly the same place next to the elevator. Finally, when no one is looking Mrs. Winkler wheels into the elevator. The door closes and the elevator takes off for the ground floor.
Antecedent: Mrs. Winkler is a curious person and always liked walking around the city for exercise. She liked exploring the different neighborhoods. She was never one to sit around doing nothing. Mrs. Winkler can propel herself independently in the wheelchair but doesn’t always understand the consequences of her decisions. The elevator is interesting and looks like fun. People keep walking by and talking to her although she doesn’t remember what they are saying.
Behavior: The door to the elevator is an interesting visual cue and Mrs. Winkler enjoys seeing people coming and going. When a door opens, it is a common reaction to pass through it. The opening door cues Mrs. Winkler to wheel into the elevator. When the door opens on the ground floor, she wheels herself out of the elevator without knowing where it leads. Her behavior is consistent with her personality and her previous habits.
Consequence: Once she gets into the elevator, Mrs. Winkler’s inability to think logically puts her at great risk. She exits the elevator next to a door that leads out of the building and wanders into the street. A concerned passerby recognizes that she needs help and takes her back to the assisted living facility.
Discussion: Mrs. Winkler doesn’t understand the danger and does not remember the warnings to stay out of the elevator. One solution is to alter the environment. Move Mrs. Winkler to a place where she cannot see or hear the elevator. Try to determine the reason for her wandering. Review her medications to make sure wandering is not the result of a medication side effect, or a drug interaction. Use the following suggestions to keep Mrs. Winkler out of the elevator:
- Redirect her to a purposeful activity.
- Provide a place where she can wander safely.
- Encourage with regular exercise.
- Ask for her help with simple, meaningful chores.
- Attach an electronic device to Mrs. Winkler’s ankle or wrist that alerts caregivers when she has wandered out of a designated area.
- Paint a grid in front of the elevator to discourage her from getting into the elevator.
- Place a plastic vertical PVC pole on the back of her wheelchair and a horizontal pole across the entrance to the elevator so that she is gently but physically stopped from entering the elevator.
- Encourage a family member to take her for a stroll outside the building or for a ride in a car.
2.3.4 Rummaging and Hoarding
Rummaging and hoarding are behaviors in which a person gathers, hides, or puts away items in a secretive and guarded manner. Memory loss, poor judgment, and confusion contribute to rummaging and hoarding. Rummaging and hoarding are not necessarily dangerous or unsafe, but these behaviors can be frustrating for caregivers.
Rummaging and hoarding are obsessive/compulsive behaviors. A person who feels a strong need to rummage or hoard can be remarkably persistent, secretive, and patient making it difficult for caregivers to address these behaviors. Hoarding is associated with insecurity, fear, anger, and the desire to hold onto possessions and memories from the past. A person who hoards may fear losing money or possessions. They may feel a lack of control or a need to “save for a rainy day”.

An older woman rummaging in her closet. Created by author using Midjourney AI.
Rummaging through familiar items can create a sense of safety and security. Confusion can lead to rummaging through another person’s belongings, which can be particularly frustrating for other people.
To address rummaging and hoarding behaviors, try to determine what triggers the behavior and look at the consequences, if any. Look for patterns and carefully observe the person’s hiding places. The reason for rummaging and hoarding may not be clear to you but there may be a perfectly good reason why someone living with dementia is rummaging.
The rummaging impulse might be satisfied by creating a rummaging room or a bag or drawer of items that the person can pick through. Rummaging through another person’s belongings can be prevented by installing locks on drawers and closets. Restricting all rummaging and hoarding can be frustrating for a person who enjoys these activities.
In facility settings, reduce clutter and label cabinets, doors, and closets (with words or pictures). Poisonous items should be stored away from common areas in locked cabinets.
2.3.5 Sleep Disturbances
Many people living with dementia experience sleep disturbances due to comorbid medical conditions and environmental factors. Common sleep problems include insomnia, fragmented sleep, obstructive sleep apnea*, rapid eye movement sleep behavior disorder**, and restless legs syndrome. Individuals may have trouble falling asleep or staying asleep due to altered circadian rhythms*** and increased confusion during the night. (Mukherjee et al., 2024).
*Obstructive sleep apnea: a syndrome caused primarily by the collapse of the upper airway during sleep.
**Rapid eye movement sleep behavior disorder: a sleep disorder in which individuals physically and/or vocally act out vivid, often unpleasant dreams and sudden, involuntary arm and leg movements during REM sleep.
***Circadian rhythms: disruption in the body’s sleep-wake cycle.
Comorbid medical conditions that can affect sleep in older adults living with dementia include:
- cardiovascular disease
- diabetes
- depression and anxiety
- thyroid disorders (hypothyroid and hyperthyroid)
- untreated or poorly treated pain
The Center for Medicaid and Medicare Services (CMS) now requires non-pharmacologic interventions for sleep disturbances be tried and documented before using sedatives or psychotropic medications in a person living with dementia (CMS, 2024).
Non-pharmacological treatments can include (Mukherjee et al., 2024; CMS, 2024):
- Cognitive-behavioral therapy for insomnia.
- Minimizing environmental disruptions (reducing nighttime noise and excessive light).
- Avoiding stimulating activities close to bedtime.
- Encouraging good sleep hygiene (a regular bedtime routine and a warm comfortable sleeping environment).
- Restricting caffeine, nicotine, and alcohol.
In addition to affecting the health and quality of life of the person living with dementia and their caregivers, sleep disturbances can contribute to challenging behaviors. CMS requires that sleep disturbances be evaluated when a person exhibits agitation, anxiety, wandering, or changes in cognition. This includes looking for potentially treatable causes such as pain and discomfort, hunger and thirst, the need to urinate, infections, and adverse drug reactions.
Sleep disturbances can lead to “sundown syndrome”, a set of symptoms or behaviors that emerge in the late afternoon or early evening. Managing sundown syndrome involves a combination of environmental, behavioral, and medical interventions. A consistent daily routine, regular physical activity, soothing and familiar activities in the late afternoon, and a calm and a comfortable environment can improve sleep and decrease sundowning (Mukherjee et al., 2024).
Benzodiazepines, which have a hypnotic, sedative effect are currently the most widely prescribed medications for sleep disorders in older adults. Despite their widespread use, concerns remain regarding their potential for tolerance, dependence, and adverse effects such as cognitive impairment (especially in older adults) (Chavez-Mendoza, 2025).
Benzodiazepine dependence has been associated with severe depression and anxiety and impaired cognitive and psychosocial function. In older adults, increased sensitivity to benzodiazepines can increase the risk of confusion, disorientation, and falls. These adverse effects increase the complexity of treating clients living with dementia (Chavez-Mendoza, 2025).
Recently, non-benzodiazepine hypnotics, commonly known as Z-drugs, have been suggested as effective alternatives due to their similar mechanism of action. They may improve sleep quality, lower dependency risks, and reduce adverse effects compared to benzodiazepines (Chavez-Mendoza, 2025).
Treating sleep disturbances involves looking for potentially treatable causes. This includes treating pain and discomfort, hunger and thirst, the need to urinate, infections, and adverse drug reactions.
Non-pharmacological treatments that can improve sleep include:
- light therapy
- exercise and individualized social activities
- caffeine, nicotine, and alcohol restriction
- comfortable beds with enough pillows for back and neck support
- good temperature control in rooms
- noise reduction
2.4. Physical and Chemical Restraints
When—if ever in the eternal dementia care merry-go-round of staff shortages, budget limitations, regulatory approvals, mandates, or penalties—will we focus on the people we are supposed to be serving without turning first to medications.
Teepa Snow, STOP Treating Behaviors with Restraining Medications
The Omnibus Budget Reconciliation Act of 1987 (OBRA 87) established a resident’s right to be free of physical or chemical restraints in nursing homes when used for the purpose of discipline or convenience and when not required to treat the resident’s medical symptoms. Uncooperativeness, restlessness, wandering, or unsociability are not sufficient reasons to justify the use of a restraint (GovTrack, 2020).
Florida law specifies that a facility must not use verbal, mental, sexual, or physical abuse, corporal punishment, or involuntary seclusion. A facility must ensure that the resident is free from physical or chemical restraints imposed for purposes of discipline or convenience and that are not required to treat the resident's medical symptoms. When the use of restraints is indicated, the facility must use the least restrictive alternative for the least amount of time and document ongoing re-evaluation of the need for restraints (FL Statutes, 2024).
The use of Posey restraints* is prohibited in assisted living facilities and congregate care settings in Florida. Other physical restraints may be used in accordance with agency rules when ordered by the resident’s physician and consented to by the resident or the resident’s representative (FL Statutes, 2024).
*Posey restraints: soft holders attached to wrists or ankles, sleeveless vests with straps attached to the chair or bed, waist and chest belts, padded mitts, and 4 or 5 point extremity restraints.
The use of a restraint must include care planning, staff monitoring, and periodic review by a physician. The use of chemical restraints is limited to prescribed dosages of medications authorized by the resident’s physician and must be consistent with the resident’s diagnosis. Residents who are receiving medications that can serve as chemical restraints must be evaluated by their physician at least annually to assess (FL Statutes, 2024):
- The continued need for the medication.
- The level of the medication in the resident’s blood.
- The need for adjustments in the prescription.
For a given client at a particular point in time, the assessment is used to determine whether the use of less restrictive measures poses a greater risk than the risk of using a restraint (FL Statutes, 2024).
The comprehensive assessment should identify medical problems that may be causing behavior changes. For example, temperature elevations, hypoxia (low levels of oxygen), hypoglycemia (low blood sugar), electrolyte imbalances, drug interactions, and drug side effects may cause confusion, agitation, and combative behaviors. Addressing these medical issues may eliminate or minimize the need for the use of restraints or seclusion (FL Statutes, 2024).
2.4.1 Physical Restraints
A physical restraint is any manual method, physical or mechanical device, material, or equipment attached to or adjacent to a person’s body that the individual cannot remove easily and which restricts freedom of movement or normal access to one’s body.
Physical restraints can include:
- belts
- mittens
- soft wrist and ankle restraints
- vest and jacket restraints
- bedrails
- geriatric chairs and recliners
- wheelchair safety bars
- lapboards
Use of physical restraints can cause agitation, confusion, deconditioning, pressure ulcers, strangulation, and even death. Restraints affect a person’s sense of well-being, causing feelings of low self-worth, depression, withdrawal, humiliation, and anger.
Restraint can include using (or threatening) force or restricting a person’s movements—even if they do not resist. Forced isolation (such as locking a person in their bedroom) is also a type of restraint.
A restraint-free environment should be the standard of care and goal for adult day care facilities. Restraint reduction programs can significantly reduce the use of restraints. Healthcare providers can lead the way by educating themselves about the dangers of restraints and sharing this knowledge with family caregivers.
Person-centered care focuses on practices that respect the dignity of each individual. Collaborating with family members and the person living with dementia allows the development of an individual care plan that addresses issues that affect a person’s safety and wellbeing.
The use of physical restraints can be reduced or eliminated by creating an environment that is friendly toward older adults, embraces aging with compassion, promotes safe mobility by making the physical environment accessible to people with disabilities, and caters for the needs of older people (Atee et al., 2023).
Restraints should not be considered a routine part of a falls-prevention program. There is no evidence that the use of physical restraint, (including, but not limited to, raised side rails) will prevent or reduce falls. Additionally, falls that occur while a person is physically restrained often result in more severe injuries. In fact, in some instances reducing the use of physical restraints actually decreases the risk of falling (CMS.gov, 2024).
2.4.2 Chemical Restraints
The term “chemical restraint” refers to the use of antipsychotic, antianxiety, antidepressant, or sedative medications for the purpose of controlling or restricting a person’s behavior or movement. Unfortunately, a decrease in the use of physical restraints has been linked to the increased use of chemical restraints (Cain et al., 2023).
In 2023, the American Geriatrics Society Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults stressed the need to avoid antipsychotics and other medications for behavioral problems of dementia and delirium because their use is frequently associated with harm (AGS, 2023).
Between 2011 and 2019, psychotropic drugs* were prescribed to about 80% of nursing home residents. Higher use of psychotropic drugs was associated with nursing homes with lower ratios of registered nurse staff to residents. Nursing homes with a higher percentage of low-income residents were also associated with higher use of these drugs (OIS, 2022).
*Psychotropic drugs: antipsychotics, anticonvulsants, mood stabilizers, and central nervous system agents.
Behavioral interventions are the preferred management strategy for treatment of challenging behaviors associated with dementia. The decision to use or not use a chemical restraint should always be made in collaboration with the client and family members (AGS, 2023).
A provider may choose to prescribe an antipsychotic medication when symptoms are severe, dangerous, or cause significant distress to the client. These medications may be effective in some cases. However, the provider must disclose to the client and family that the medication is being used off-label* meaning a drug has not been approved by the Food and Drug Administration (FDA) for treatment of behavioral symptoms of dementia. The provider must obtain permission from the client or family member to use these drugs for behavioral symptoms of dementia.
*Off-label: prescribing medications for an unapproved indication, age group, dose, or form of administration.
2.4.3 Alternatives to Restraints
There are many alternatives to the use of physical and chemical restraints. Some alternatives enhance safety and comfort for all residents, such as increasing staffing levels, removing hazards, providing safe areas for walking, and training staff on how to identify and respond to unmet needs (CANHR, 2025).
Other alternatives include adapting and tailoring chairs to improve comfort and safety, using pads and pillows to support comfortable and safe body positions, providing therapy and restorative care to improve a resident’s ability to move about safely, adjusting care and caregiver assignments to a resident’s preferences, and using low beds and floor padding to safeguard against harmful falls from bed (CANHR, 2025).
Establishing a routine, including a toileting schedule, prevents mad dashes to the bathroom that increase the risk of falls. Regular exercise, a comfortable place to rest, and a schedule for napping can also help. On a regular basis:
- Address hunger, thirst, and discomfort.
- Review medications for adverse effects.
- Treat all underlying causes, including pain.
- Assess hearing and vision.
- Relieve impaction.
An uncluttered environment can reduce the need for physical restraints. Hallways, common areas, and resident rooms should be free of equipment and obstacles. Providing wall rails, grab bars, and transfer poles in rooms, bathrooms, hallways, and common areas promotes independence reduces caregiver stress and worry.