*This course has been retired. Please click here for new course, About Suicide: Washington State, 6 units.
In the United States and throughout the world, suicide is a major public health concern. In 2015, 44,000 Americans died from suicide, making it the tenth leading cause of death overall. And suicide is not limited to any gender, age, socioeconomic, or ethnic group. Among children (age 10 to 14), suicide is the third leading cause of death, while among older teenagers and young adults (age 15 to 34), suicide is the second leading cause of death. Remarkably, in 2015 there were many more suicides (44,193) in the United States than homicides (17,793) (CDC, 2017).
Suicide Rates in the United States
(by state; per 100,000; average 2004–2010)
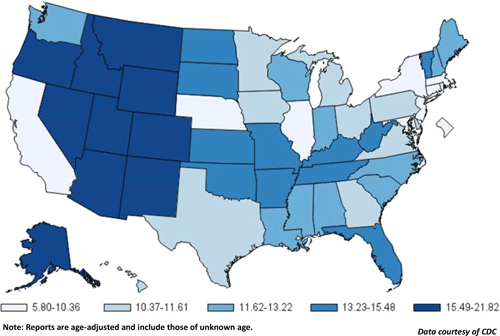
Suicide rates vary from state to state. Washington State, as well as other Western states (excluding California), have some of the highest rates of suicide in the country. Source: CDC.
A web of biological, psychological, social, environmental, and situational concerns influence suicidal ideation and behaviors. Risk factors, including childhood trauma, substance abuse, poverty, and untreated mental health problems, are common. Unfortunately, many people cannot get help because of provider shortages, stigma associated with mental illness, and the cost of care (WSDOH, 2016).
Although men have a higher rate of completed suicides, suicide attempts are two- to three-fold more frequent among women. Methods are also different: men often use lethal methods such as firearms, hanging, or suffocation, while women attempt suicide by poisoning, wrist cutting, or falling from heights (Mendez-Bustos et al., 2013).
Prevalence of Suicide Attempts Among U.S. Adults (2015)

Defining Terms
- Suicide is defined as death caused by self-directed injurious behavior with intent to die as a result of the behavior.
- A suicide attempt is a non-fatal, self-directed, potentially injurious behavior with intent to die as a result of the behavior. A suicide attempt might not result in injury.
- A suicidal ideation refers to thinking about, considering, or planning suicide.
Source: CDC, 2016.
In Washington State the suicide rate is 11% higher than the national average; from 2010 to 2014, over 5,000 people died as a result of suicide. Three Washingtonians die by suicide every day and in an average week there are 65 hospitalizations from self-inflicted injury. More than 4% of adults and 20% of 10th graders in Washington seriously considered suicide in the past year (WSDOH, 2016).
Suicide rates vary in different parts of Washington. But because of the way rates are compared, a small difference may be statistically significant while a larger one is not. Statistical significance means the difference is very unlikely to be due to chance. From 2010 to 2014, suicide rates were higher than the state rate in six counties:
- Clallam
- Grays Harbor
- Okanogan,
- Pierce
- Skamania
- Stevens (WSDOH, 2016)
Seven counties in Washington have small populations and had too few suicides to calculate a suicide rate. This does not mean that there are not suicides in these counties; county-level data do not always accurately reflect suicide losses in communities. For example, in 2013 both the Spokane Tribe of Indians and the Colville Confederated Tribes declared a suicide state of emergency because of high numbers of suicide deaths. Clark County’s Battle Ground School District, located in a town of fewer than 18,000 residents, lost seven students to suicide between 2011 and 2013. Neither pattern of loss was clear from a glance at county data. In Washington and nationally, suicide rates are higher outside urban areas and highest in small-town rural areas (WSDOH, 2016). The suicide rate in King County is lower than the state rate, but it has the largest population and the highest number of suicides in the state (WSDOH, 2016).
2008–2014, Washington Death Rates per 100,000 Population

Produced by: the Statistics, Programming & Economics Branch, National Center for Injury Prevention & Control, CDC.
Data sources: NCES National Vital Statistics System for numbers of deaths; US Census Bureau for population estimates.
Key Points about Suicide
- Suicide is a preventable public health problem, not a personal weakness or family failure.
- Everyone in Washington has a role in suicide prevention; suicide prevention is not the responsibility of the health system alone.
- Many people avoid discussing suicide; silence and stigma harm individuals, families, and communities.
- To prevent suicide in Washington, we must change the factors that contribute to suicide risk, such as childhood trauma, isolation in our communities, access to lethal means, and lack of access to appropriate behavioral healthcare.
- Suicide does not affect all communities equally or in the same way; suicide prevention programs should be based on the best available research and practices, while reflecting community needs and local cultures.
- People experiencing mental illness, substance use disorders (SUDs), trauma, loss, and suicidal thinking and behavior deserve dignity, respect, and the right to make decisions about their care.
Source: Washington State Department of Health, 2016.
Suicide, Race, and Ethnicity
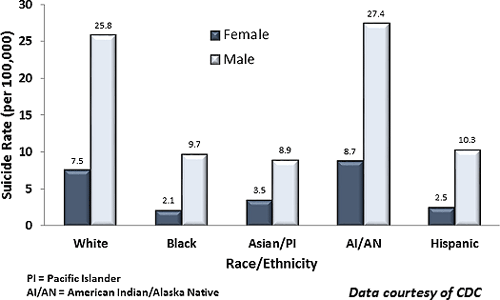
Suicide rates in Washington are highest among American Indian, Alaska Native, and white populations, consistent with national rates. But these broad demographic groups are diverse with regard to national origin and ethnicity, which can mask the impact of suicide in different subgroups. For example, the broad Asian population’s overall low suicide rate may hide the high impact of suicide in some Asian ethnic groups.
American Indians and Alaska Natives face severe historical trauma, high rates of poverty and isolation, cultural taboos around death and suicide, and lack of access to mental healthcare. Among American Indian and Alaska Native youth aged 15 to 24 years, the suicide rate is 3 to 4 times higher than other American youth and is the second leading cause of death for American Indian and Alaska Natives in this age group (WSDOH, 2016). The risk for co-occurrence of substance abuse, depression, and diabetes is over 12 times higher for AI/ANs than for whites (Cwik et al., 2016). The suicide rate for American Indian juveniles is more than double the white non-Hispanic rate and more than triple the rates for the other racial/ethnic groups (CSAT, 2015).
Very little research focuses on why suicide rates are high among white populations. Centers for Disease Control and Prevention (CDC) data from 16 states show the most common circumstances around suicide for white men include mental and physical health problems, trouble in intimate relationships, alcohol dependence, and problems at work. Cultural taboos about seeking help and appearing vulnerable can isolate white men from both support systems and resources that could help (WSDOH, 2016).
Hispanics/Latinos have fairly similar rates of suicidal thoughts and behaviors compared with white, non-Hispanic individuals. Among youth and young adults, the prevalence of suicidal thoughts and behavior increases among Hispanics/Latinos who are more acculturated to mainstream American culture, particularly among females (CSAT, 2015).
The suicide rate for African Americans is 70% lower than that of the non-Hispanic white population. However, in 2014 the suicide death rate for African Americans men was more than four times greater than for African American women (OMH, 2017).
Among African American youth, suicide risk peaks in early twenties for males and late twenties for females. These patterns are very different from the age patterns of the white population and the whole population. In a study looking at suicide rates from 1983 to 2012 for African Americans, the risk of suicide in both genders showed a similar trend: the risk in males increased with age peaking at ages 20 to 24 years and then declined except for slight increases at older ages (60–74 years). For females, the risk increased with age until peaking at ages 25 to 29 years and then declined except for slight increases at middle ages (35–44 years) (Wang et al., 2016).
Among Asian American the six largest subgroups in the United States are Asian Indians, Chinese, Filipinos, Japanese, Koreans, and Vietnamese; these subgroups account for 84% of all Asian Americans in the United States. Among these Asian subgroups, Korean males had more than twice the frequency of death due to suicide (5%) compared to non-Hispanic Whites (2%), and suicide was ranked as the fifth leading cause of death, higher than every other Asian subgroup and non-Hispanic whites. Mortality rates for suicide among Korean males were twice that of any other Asian subgroup (Hastings et al., 2015).
Suicide Rates by Race/Ethnicity in the United States (2014)
Suicide vs. Homicide
For white youth and young adults between the ages of 12 and 24, between 1990 and 2015 suicide was much more common than murder. This was in sharp contrast to patterns for Hispanics and non-Hispanic blacks. For white youth between the ages of 7 and 17, for every 10 homicide victims there were 29 suicide victims. For black youth, for every 10 homicide victims there were to 2 suicide victims. For Hispanic youth, for every 10 homicide victims, there were 5 suicide victims (OJJDP, 2017).
Whites: Number of Suicide and Homicide Victims by Age, 1990–2015
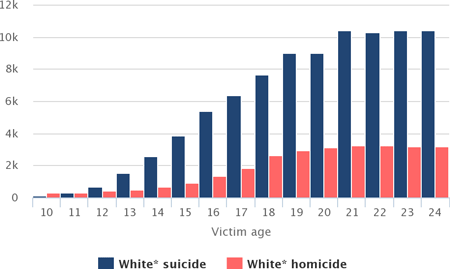
Source: Office of Juvenile Justice and Delinquency Prevention, 2017.
Blacks: Number of Suicide and Homicide Victims by Age, 1990–2015
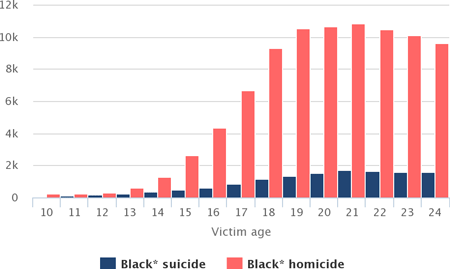
Source: Office of Juvenile Justice and Delinquency Prevention, 2017.
Hispanics: Number of Suicide and Homicide Victims by Age, 1990–2015
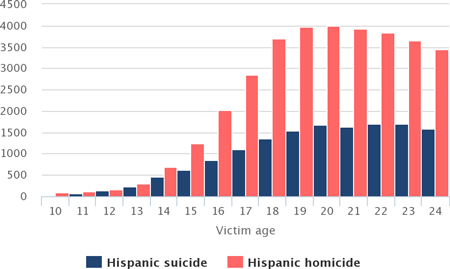
Source: Office of Juvenile Justice and Delinquency Prevention, 2017.
In contrast, the suicide rate for American Indian juveniles (69.8) was more than double the white non-Hispanic rate and more than triple the rates for the other racial/ethnic groups. Hispanics/Latinos have fairly similar rates of suicidal thoughts and behavior compared with white, non-Hispanic individuals. Among youth and young adults, the prevalence of suicidal thoughts and behavior increases among Hispanics/Latinos who are more acculturated to mainstream American culture, particularly among females (CSAT, 2015).
Gender and Age Differences
Suicides of young people receive a lot of media and community attention, though Washington’s suicide rates for adults are higher. Men are more likely to die by suicide than women, but women are more likely to attempt suicide. Men are more likely to use deadlier methods, such as firearms or suffocation. Women are more likely than men to attempt suicide by poisoning (WSDOH, 2016).
During 2012–2014, 77% of suicide deaths in Washington were males. Men 75 and older had the highest rate, while men 45 to 64 had the highest total number of suicides. National data linked the recent economic recession to increases in middle-aged adult suicides, showing that external economic factors were involved in 37% of suicides. For elderly men, contributing factors include economic insecurity, loss of significant relationships, loneliness, fear of being a burden, and the physical and mental stresses of aging (WSDOH, 2016).
Suicide Rates by Age in the United States (2014)

In men, signs of suicidal ideation include social withdrawal, anger, and reduced problem solving capacity. Signs of suicide attempt include statements of suicidal intent, calmness, anger, apathy, hopelessness, risk-taking, and appearing “at peace.” Signs preceding death by suicide include desperation and frustration in the face of unsolvable problems, helplessness, worthlessness, statements of suicidal intent, and emergence of a positive mood state (Hunt et al., 2017).
Among women in the United States, suicide is concentrated in the 35 to 64 years age group (64.8%), peaking among women aged 45 to 54 years. From 50 years of age, the suicide rates among women tend to diminish progressively, until old age, when rates start increasing again (Mendez-Bustos et al., 2013).
Case
A 69-year-old Caucasian man—a retired builder with a medical history of chronic depression—was brought to hospital after a failed suicide attempt. The attempt consisted of self-asphyxiation with car exhaust fumes and shooting himself three times with a three-inch nail gun. The initial shot was directed upward through the submental triangle behind the chin. It pierced his tongue, upper denture plate, and hard palate, effectively pinning his mouth shut. The subsequent two shots were fired into the fourth intercostal space immediately left of the sternum.
On admission to the emergency department the patient was distressed but hemodynamically stable. An examination revealed nail gun entry wounds on his left anterior chest wall over the precordial area, and at the submandibular area under his chin, pinning his mouth closed. The nails within the thorax could not be confidently located on chest X-ray; however, transthoracic echocardiography suggested a nail had possibly penetrated into the right ventricle. There was no associated pericardial effusion. In light of the potential for rapid deterioration, the patient was immediately transferred to the operating room where preparations for an exploratory midline sternotomy and thoracotomy were made.
The potential for rapid hemodynamic deterioration due to the intrathoracic penetrating injury required urgent surgical exploration. The uncertainty in the location of the intrathoracic nails meant the exact nature of the surgical repair was not defined and provision for lung separation needed to be planned for. In this case, the chest x-ray failed to allow an adequate view of the nail within the thorax. Although transthoracic echocardiography suggested the nail had penetrated the right ventricle, the exact location of the nail was not clear.
Cardiopulmonary bypass was initiated to facilitate surgical exposure. During cardiopulmonary bypass the endobronchial balloon was deflated, as lung isolation was not required, and cardiac repair was completed uneventfully. Removal of the nail from his mouth required a small incision into the hard palate and extraction using surgical pliers, removing the nail from his hard palate, upper denture, and tongue. The patient made an excellent recovery and was discharged five days later to a psychiatric community hospital for ongoing psychological rehabilitation.
Source: Lim et al., 2013.