1. Understanding Alzheimer’s Disease and Related Disorders (ADRD)
Alzheimer’s disease and other types of dementia cause damage to the entire brain. It affects memory, thinking, emotions, judgment, reasoning, social skills, and a person’s ability to function in daily life. Dementia occurs primarily in later adulthood and is a major cause of disability in older adults. Although almost everyone living with dementia is older, dementia is not considered a normal part of aging.
1.1 Defining Dementia
Dementia is a term used to describe a group of symptoms that damage brain cells. Alzheimer’s disease and most other types of dementia are progressive, and symptoms worsen over time as brain cells die. meaning damage gets worse over time. Dementia is a terminal illness, eventually leading to death.
Dementia affects our executive functions; the skills we need to manage our daily lives. The gradual loss of executive functions makes it hard to plan for the future, follow complex conversations, remember new things, and control our emotions.
Alzheimer’s disease and other types of dementia cause damage to a part of the brain called the cerebrum. The cerebrum fills up most of our skull and is divided into four lobes (or segments, one on each side of the head):
Frontal (right behind your forehead)
Temporal (on the side of your head above your ears)
Parietal (in the middle of your head above the temporal lobes)
Occipital (at the back of your head)
The cerebrum allows us to understand the world around us. It controls our memories and emotions. It helps us to reason, make decisions, and tell right from wrong. It also controls our movements, vision, and hearing. Many of these areas of the brain are damaged by dementia.
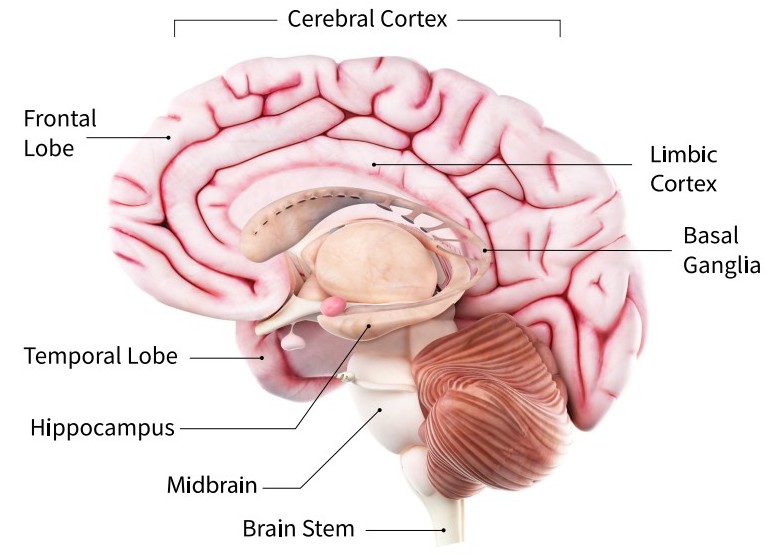
The Human Brain

The four lobes of the cerebrum, plus the cerebellum and the brainstem. Alzheimer’s disease starts in the temporal lobe, an area of the brain associated with memories and emotions. (Copyright, Zygote Media Group, Inc. Used with permission.)
When someone has dementia, their thinking gradually becomes less clear. Decisions are more difficult and safety awareness declines. People also get tired more easily. People living with Alzheimer’s disease and other types of dementia sometimes have difficulty controlling their emotions.
After the age of 55, the risk of developing dementia increases. Between the ages of 55 and 75, the risk is relatively low (4%). After the age of 75 the risk increases, with the highest risk occurring in people over the age of 85. Certain groups have greater risks than others. For example, women have a higher lifetime risk due to survival to older ages than men (Fang et al., 2025).
The term ADRD (Alzheimer’s disease and related dementias) is a general one that refers to more than one type of dementia. While Alzheimer’s disease is the most common dementia diagnosis, other types of dementia share many features with Alzheimer’s. More often than not, patients with a clinical diagnosis of Alzheimer’s disease have mixes of brain pathologies, complicating both diagnosis and treatment (NINDS, 2025, December 12).
1.2 Defining Alzheimer’s Disease and ADRD
Alzheimer’s disease (AD) is the most common kind of dementia. It typically starts in an area of the brain called the hippocampus. This is the part of the brain responsible for regulating emotions, forming new (short-term) memories, and converting these memories for later use (long-term memories).
Damage to this part of the brain can cause a person to forget something that happened just a moment ago. The following pictures show how damage from Alzheimer’s dementia gradually spreads throughout the brain.
Brain Changes in Mild Dementia

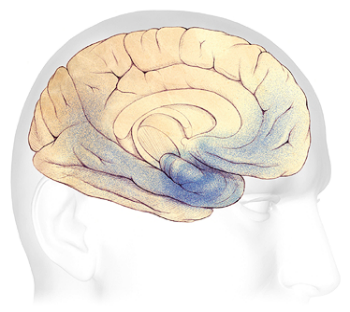
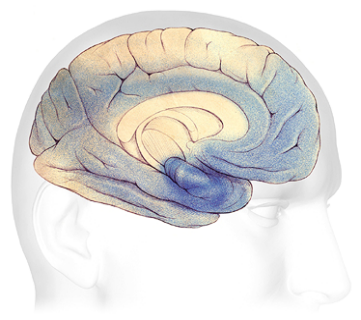
In the early stage of Alzheimer’s disease, “plaques” and “tangles” (clumps) form in and around the hippocampus (shaded in blue). In the moderate stage, damage spreads from the hippocampus forward to the frontal lobes. In advanced Alzheimer’s, plaques and tangles have spread throughout the entire brain. (Source: The Alzheimer’s Association. Used with permission.)
Normal Brain Contrasted with AD Brain
A view of how Alzheimer’s disease changes the whole brain. Left side: normal brain; right side, a brain damaged by advanced AD. (Courtesy of The Alzheimer’s Association. Used with permission.)
1.3 Other Types of Dementia
Although Alzheimer’s dementia gradually worsens over time, other types of dementia can progress differently.
1.3.1 Vascular Dementia
Vascular dementia is related to cerebrovascular disease. It can be caused by any disease or disorder that damages the vessels supplying blood to the brain. This can include hypertension, heart rhythm irregularities, diabetes, high cholesterol, smoking, sleep-disordered breathing, and a sedentary lifestyle.
Vascular dementia usually has a stepwise onset, meaning symptoms can stay the same for a long period of time, then suddenly worsen. Memory may be less affected than in Alzheimer’s disease, while fluctuations in mood are more common. Cognitive impairment is often “patchy” because of small vessel damage throughout the brain.
Although Alzheimer’s disease is the most common cause of dementia, vascular cognitive impairment and vascular dementia represent the second leading cause, accounting for approximately 15% to 20% of all dementia cases (Yang, 2025).
1.3.2 Lewy Body Dementia
Lewy body dementia (LBD) is progressive (symptoms start slowly and worsen over time). Early symptoms can include changes in mood, vision, sleep, and bowel movement dysfunction. Nervous system tissue outside the brain, including nerves in the intestines, heart, sex organs, and salivary glands, can be affected by LBD as well. This may lead to symptoms such as constipation, dizziness with changing position, sexual dysfunction, or drooling (NIA, 2025, January 27). Symptoms often fluctuate, even throughout the course of the day.
Lewy bodies are made of a protein called alpha-synuclein. In LBD, alpha-synuclein forms into clumps inside nerve cells, starting in specific regions of the brain. This process causes nerves to weaken and, eventually, to die. The result is widespread damage to certain parts of the brain and a decline in abilities controlled by the affected brain regions (NIA, 2025, January 27).
LBD dementia affects many parts of the brain including those shown above. Source: NIA, 2025, public domain.
from https://www.nia.nih.gov/health/lewy-body-dementia/lewy-body-dementia-causes-symptoms-and-diagnosis
Lewy body dementia lasts an average of 5 to 7 years from the time of diagnosis to death, but it can range from 2 to 20 years. How quickly symptoms develop varies greatly from person to person, depending on overall health, age, and severity of symptoms (NIA, 2025, January 27).
Parkinson’s disease dementia is a form of LBD. People with either form of LBD eventually develop similar symptoms due to the presence of Lewy bodies in the brain. But there are some differences. For example, the symptoms of dementia with Lewy bodies may worsen more quickly than those of Parkinson’s disease dementia (NIA, 2025, January 27).
1.3.3 Frontotemporal Dementia
Frontotemporal dementia (FTD) is caused by damage to nerve cells primarily in the frontal and temporal lobes of the brain. As nerve cells die in these regions, the frontal and temporal lobes atrophy, or shrink. Gradually, this damage causes difficulties in thinking and behaviors normally controlled by these parts of the brain (NIA, 2025, January 22).
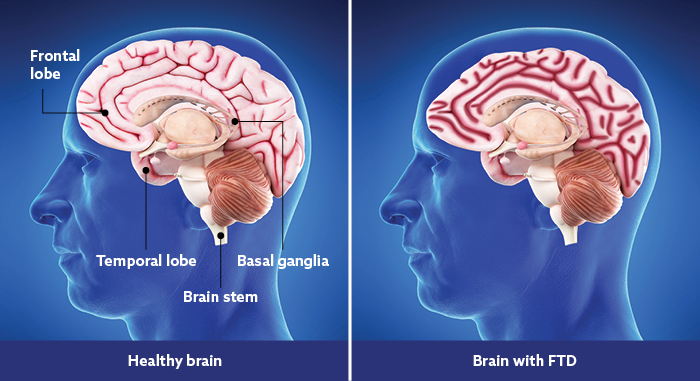
An illustration showing the location of the frontal and temporals lobes of the brain. Note the shrinkage of brain tissue in the right picture. Source: NIA, 2025, public domain.
Frontal-temporal dementia usually starts at an earlier age than Alzheimer’s disease. Depending on which side of the brain is affected, there are changes in personality, behavior, emotions, and judgment. There may also be early changes in language ability, including speaking, understanding, reading, and writing.
For caregivers and healthcare providers, one of the most striking and difficult aspects of frontotemporal dementia is the sometimes profound personality changes that can occur in a person experiencing the effects of damage to this part of the brain. The front part of the brain controls impulses, mood, ethical decisions, and compulsive behaviors. A person living with FTD may engage in verbal, physical, or sexual behaviors that are socially unacceptable and that never occurred prior to the onset of dementia. This is because of the loss of inhibition and emotional control due to damage to front part of the brain.
Motor (movement) decline can also occur as FTD progresses. A person may experience difficulties with movement, including the use of one or more limbs, shaking, difficulty walking, frequent falls, and poor coordination. Apathy, an unwillingness to talk, dramatic overeating, and depression are also common.
1.4 How ADRD Differs from Normal Aging
We all experience changes as we age. Some people become forgetful when they get older. They may forget names or titles. They may forget where they left their keys. They may also take longer to do certain mental tasks. They may not think as quickly as they did when they were younger. These are called age-related changes. This is a normal part of aging—it is not dementia.
People experiencing age-related changes can do everything in their daily lives—they can prepare their own meals, manage their finances, safely drive a car, go shopping, and use a computer. They understand when they are in danger and know how to take care of themselves. Even though they might not think or move as easily or quickly as when they were young, their thinking is normal—they do not have dementia.
In some older adults, memory problems are a bit worse than normal age-related changes. This is known as mild cognitive disorder (trouble thinking clearly). Mild cognitive disorder isn’t dementia. You won’t generally see personality changes, just a little more difficulty than is normal with thinking and memory. For some people, however, mild cognitive disorder gets worse and can develop into dementia.
Mild cognitive changes do not always develop into dementia. A person with mild cognitive impairment may remain at this level or even revert back to normal cognition under certain circumstances.
Here are some of the differences between someone who is aging normally and someone who shows the effects of dementia.
1.5 Conditions That Can Mimic Dementia
There are many conditions that can cause symptoms that look like dementia. Some conditions—infections; constipation; reactions to or interactions between medications; and abuse of alcohol, prescription medications, or recreational drugs—can be reversed with treatment.
Medical conditions other than dementia can cause cognitive changes in older adults. Gerontology specialists speak of the “3Ds”—Dementia, Delirium, and Depression—because these conditions are common reasons for cognitive changes in older adults. Delirium and depression can often be mistaken for dementia.
1.5.1 Delirium
Delirium is sudden, severe confusion with rapid changes in brain function. Along with dementia, it is a common cause of altered (changed) mental status in older adults (Jandu et al., 2025). Delirium has an abrupt onset, developing over hours or days and is typically temporary and reversible.
Delirium and dementia can occur together. Delirium is often confused with depression or dementia. Many common causes of delirium are reversible, so recognizing signs of delirium can lead to rapid improvement.
The most common causes of delirium in people with dementia are medication side effects; low or high blood sugar; fecal impactions; urinary retention; electrolyte disorders and dehydration; infection; stress; and metabolic changes. An unfamiliar environment, injury, or severe pain can also cause delirium. As a care provider who has direct daily contact with a client, your observations and feedback help other healthcare providers to identify changes that may be treatable.
1.5.2 Depression
Depression is a common but serious mood disorder. It is very common in people living with dementia and may be unseen and therefore not diagnoses or treated.
Major depressive disorder can interfere with a person's ability to sleep, eat, exercise, and participate in activities. Some people may have only a single episode within their lifetime, but more often a person may have multiple episodes (NIMH, 2024).
Persistent depressive disorder (also called dysthymia or dysthymic disorder) is long-lasting (2 years or longer). Depression with symptoms of psychosis occurs when a person has severe depression, plus some form of psychosis—such as delusions or hallucinations (NIMH, 2024).
Depression in a person living with dementia is associated with decreased quality of life, faster cognitive decline, increased mortality, and increased caregiver stress. Because of this, the diagnosis and treatment of depression in people living with dementia should be a priority (O’Sullivan et al., 2022).
Depression can cause a person to feel hopeless, worthless, or helpless. Because these symptoms often overlap with cognitive decline, caregivers may fail to recognize the difference between symptoms of depression and dementia and therefore offer no treatment (NIA, 2025, February 5).
1.5.3 Medical Conditions That Can Mimic Dementia
Other conditions that can look like dementia are more complicated and usually require additional evaluation and testing. This includes head injuries from falls, subdural hematomas,* nutritional or fluid deficiencies, dehydration, and malnutrition.
*Subdural hematoma: when blood accumulates in the outer layer of the brain, usually from some sort of head injury.
Potentially treatable conditions that can affect a person’s thinking include:
metabolic, autoimmune, or endocrine abnormalities
dehydration and malnutrition
poisoning from exposure to lead, heavy metals, or other poisonous substances
brain tumors, space-occupying lesions, and hydrocephalus (fluid in the brain)
hypoxia or anoxia (not enough oxygen)
epilepsy
sleep apnea (NINDS, 2025, October 20)
1.6 Possible Causes of Alzheimer’s Disease and Other Types of Dementia
In Alzheimer’s disease, damage is thought to be caused by two abnormal proteins,* called tau and beta-amyloid, that accumulate in the brain. The proteins form “plaques” and “tangles”(clumps) inside the nerve cells and in the areas between the nerve cells.
*Abnormal proteins: complex molecules that clump or fold together, disrupting normal cell function.
But abnormal proteins may not be the only factors involved in Alzheimer’s. Other changes that affect the brain may also play a role:
lack of sufficient blood and nutrients to the brain
lack of glucose (sugar)
chronic inflammation
Risk factors associated with the development of dementia include high blood pressure, heart disease, diabetes, stroke, and Parkinson’s disease. Lifestyle risk factors include smoking, drinking large amounts of alcohol, head injuries, poor diet, and lack of exercise. Genetics also plays a role—the chance of developing a genetically linked form of dementia increases when more than one family member has the disorder (NINDS, 2025, October 20). Although genetic factors increase risk, they do not determine outcome.